We believe you can go further and do more when you have a trusted risk-discussion partner on your team, who will look at your business holistically to uncover new opportunities.
We are a leading global reinsurer that helps insurance companies reduce their earnings volatility, strengthen their capital and grow their businesses through reinsurance solutions.
A quick and easy blood draw, non-invasive, to screen someone for a wide range of cancers – this is the exciting promise of multi-cancer early detection (MCED) tests. While still in clinical trials, these tests are seen to be much closer to clinical use than previously thought, and are expected to complement, rather than replace, current cancer detection options. This was the outlook a year ago. So, where do we stand today? How close are we to having these tests available?
In this interview, PartnerRe’s Chief Medical Officer Europe and Asia Pacific, Dr. Achim Regenauer, looks at the current status of MCED tests, the multiple steps needed to make them commercially viable, and the implications for the life reinsurance business.
Q: MCED tests are set to revolutionize cancer medicine with potential impacts on the life reinsurance business. How do these tests work, and how are they different from liquid biopsies?
AR: “Liquid biopsy” is an umbrella term for testing for one specific cancer using a noninvasive blood draw rather than tissue samples. These tests look for telltale biomarkers such as DNA or other fragments that dying cancer cells release into the bloodstream. The technique has its applications in every phase of clinical cancer care, from screening for one type of tumor to diagnosing and staging it, assessing its response to treatment, and monitoring for any recurrence of growths (surveillance) post-treatment. So far, however, routine clinical use of liquid biopsy tests has been limited to assessing and surveilling a few targeted cancers individually.
Multi-cancer early detection (MCED) tests, by contrast, are intended to screen for many types of cancers all at once, usually long before the first symptoms turn up. The corresponding biomarkers can be detected in a single sample draw of blood or in other bodily fluids such as urine[1].
Q: With which types of cancer are screenings most effective?
AR: Screening for multiple types of cancer at once is a major shift from screening for just one. Selecting which cancers to screen for – the deadliest kind, the most frequently occurring or those most amenable to early therapy – is a tough call to make, even for experts. When taking this extraordinarily complex decision, we should consider three important aspects.
Screening by cancer type
The first questions to ask are: Can early detection reduce both the mortality and the morbidity of the cancers we screen for? Are the cancers prevalent enough in the population to justify the costs of testing for them? Is there an effective therapy available for them? How do we avoid overdiagnosis and overtreatment? And at what intervals should we retest?
The latter is particularly challenging, as the retesting interval will vary by type of cancer. Of the fifty kinds of tumors detected in the Galleri test[2], for example, no two are alike in growth rate or aggressiveness. Fast-growing ones usually become symptomatic early on and require shorter screening intervals for timely detection and efficient treatment. More indolent tumors, by contrast, are slow-growing and present asymptomatically in the body for a much longer time, i.e., screening intervals could be longer.
The challenge, though, is that we have no clear picture of the growth rates of many of these fifty cancers. Most of what is known about their natural histories — when they start and how quickly they progress in the absence of any intervention — is limited to the few cancers for which useful screening tests are currently available (i.e. mammograms for breast cancer, colonoscopies for colorectal cancer, pap smears for cervical cancer, chest x-ray for lung cancer, PSA tests for prostate cancer). It is entirely for this reason that we have even learned about how these particular cancers evolve during their early stages.
Determining how to deploy MCED tests is more complex because the various target cancers may have different preferred strategies. An MCED test offered annually may not have the same harm/benefit tradeoff as one offered every few years.
Screening by test
A good screening test should be able to identify a high proportion of cases with cancer, which is important for early detection (high sensitivity). MCED tests generally show increasing sensitivity as cancers advance and shed more cancer cells into the bloodstream. However, it is at the initial stages that cancers can be treated most efficiently or even cured. While MCED tests are intended for use with symptom-free individuals and would detect a higher proportion of early-stage cancers, they would also, though to a lesser degree, detect advanced stage cancers as well.
But high sensitivity can result in false positives, where the test identifies cancer that is not present. To minimize the risk of false positives, we also need high specificity, where the test can correctly identify cases without cancer.
The optimal screening approach would aim for both high sensitivity and high specificity but achieving both concurrently is impossible. In addition, MCED screening for many cancers simultaneously – while also seeking to detect them all at the earliest possible stage – may prove an elusive goal. Moreover, the MCED test should be inexpensive enough to be viable for mass screening, and ideally should be able to localize the tumor in the body.
Here, we look at the positive predictive value, or PPV. This is the likelihood that someone with a positive test result actually has a particular type of cancer, which obviously is linked to the frequency of this cancer in the general population (prevalence). A high PPV of a test is essential to reduce unnecessary diagnostic workups and the psychological and economic burden they invariably involve. On balance, it comes down to how we define the target population that stands to benefit the most from MCED testing. In addition, for testing to make sense, people need access to follow-up medical care and be willing to comply with subsequent diagnostics and therapy.
Q: Let’s say an MCED test has been developed that reasonably meets the above aspects. Would this test be ready for use, under real-world conditions?
AR: No, not entirely. There are too many questions around the consequences of testing that we still cannot answer.
The biggest challenge with MCED testing is that diagnostic and therapeutic follow-up procedures have yet to be defined for each single cancer. This will be the scenario facing patients themselves but also clinicians and private payers/insurers for individuals who initially have been tested positive for cancer. The undefined procedures add to concerns about the clinical and psychological harms as well as unnecessary costs of false positives, overdiagnosis, and overtreatment.
Take the hypothetical case of a positive MCED test indicating lung cancer. What should be done if the tumor is too small to be detected by chest CT imaging? The threshold for detection is around 2 mm. So, the cancer signal found in this instance may be a false positive, or the cancer may take more time to grow before it is detectable. What should be done about the cancer once it is detected but the patient has no symptoms? Is watchful waiting the correct course of action, or is it preemptive therapy? If it is the latter, should it be surgery, radiation, chemotherapy, or immunotherapy or a combination? Which drug, which dosage, how many cycles? And so on and so forth.
This is a unique situation which clinical medicine is still unfamiliar with. In any case, many diagnostic and therapeutic follow-up consultations await patients. This may pose a significant dilemma for them, as even with MCED screenings fully covered they still face high out-of-pocket expenses for follow-up diagnostic procedures.
More importantly still, there is no standard approach for all cancers. What approach to take will vary by cancer location (site), histologic subtype and stage, resulting in a rather sophisticated procedure. Finding the best possible and most feasible approach will require a multidisciplinary effort by clinicians, researchers, epidemiologists, data scientists, behavioral scientists, IT experts, and specialists in other fields.[3]
Q: How do you assess the economics of MCED testing – What will it take to make MCED tests commercially viable?
AR: MCED tests represent an entirely novel approach in screening many cancers with one brush stroke. Therefore, it is going to be determined by a number of factors, from defining whom to screen and for what cancer, to how to diagnose and treat any cancer found, and how often to retest, as I mentioned earlier. And then, ideally, MCED tests should capture the full economic value of ruling in and ruling out cancer. First, regulators will need to approve the tests, and, in the best-case scenario, health insurers will cover both the costs of the MCED tests and any clinical workups.
As a physician, I should only comment from a medical and insurance vantage point. Basically, tests need to be reasonably priced to be accessible for a general population. If a test is expensive and patients are left to pay for all or much of it out-of-pocket, there will be less demand for it. However, this comes down to a cost-benefit analysis of screening a target population, and is far less about cost per se.
Key considerations for cost-benefit analysis[4] include:
How often are the various cancers detected at an earlier stage compare with the standard of care (downstaging effect)?
What might be the impact of MCED testing on health outcomes, including life expectancy and quality-adjusted life expectancy?
What are the implications for medical care costs for cancers detected via MCED testing versus conventional screening?
How affordable are MCED screening tests in terms of the short-term financial impact of adding them to the current screening paradigm?
What retesting interval is best and most efficient when more frequent testing may detect more cancers?
Furthermore, the cost of MCED tests (about USD 1,000 each for a Galleri test, for example), the scope of cancers to be detected (50 in the case of Galleri), their frequency (incidence) and particularly their improvement of mortalities are additional core factors deciding who should be tested and how often.
However, I would like to emphasize that any estimate of the potential aggregate effects of an MCED test will necessarily also be based on generally accepted assumptions about a cancer’s natural history. Again, this is because hard data on all, but a few cancers is still hard to come by (see paragraph on “Screening by cancer type” above). An example of this complex calculation of health economic cost/benefit tradeoffs associated with using an MCED test can be read here.[5]
Q: For an MCED test to be commercially viable, regulators must first approve it and insurers must reimburse it. Where are we on that front?
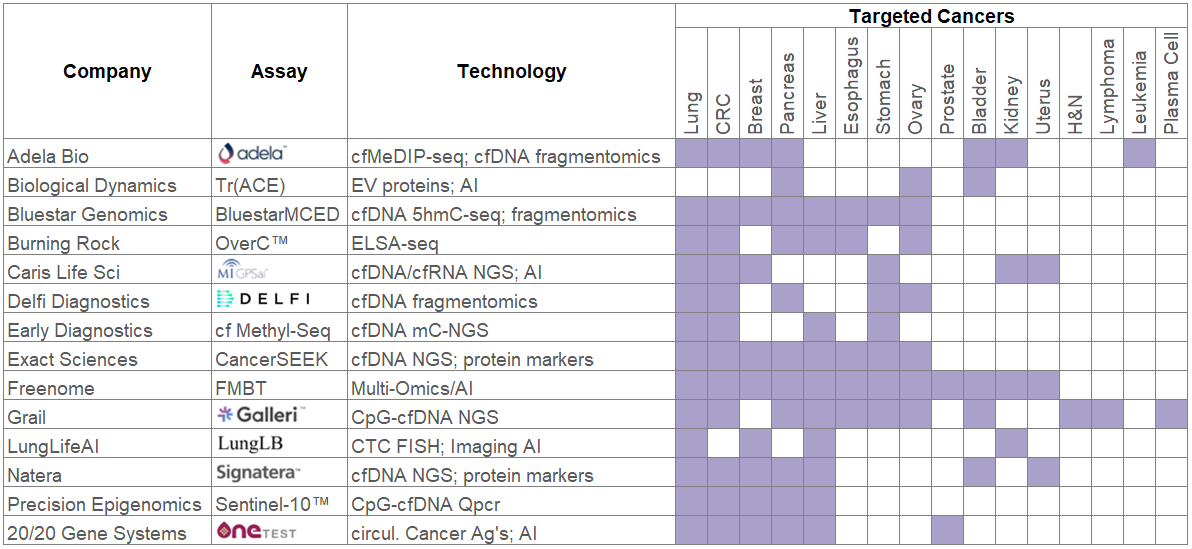
AR: Of at least a dozen MCED assays in development in the US last year (refer to Figure 1 below)[6], the Galleri test by GRAIL is the most advanced in clinical trials in the US and the UK, where a large-scale study launched in July 2022 in partnership with the National Health Service (NHS)[7].
In the US, where GRAIL is believed to seek regulatory (FDA) approval for Galleri in 2023, the test is currently available with a prescription under special regulations ((Clinical Laboratory Improvement Amendments or CLIA)[8], in partnership with various health systems and life insurers[9] [10] [11].
Fig. 1: Examples of MCED tests in the U.S
In the meantime, use of the Galleri test is limited to the US and the UK, under strictly defined experimental conditions. GRAIL is approaching reinsurers for partnerships that also include direct life insurers and third-party administrators (TPAs), with the goal of subsidizing the tests and materializing potential mortality improvements
Although no test has regulatory approval yet, the FDA does not currently enforce its regulations on MCED tests that are developed, made and processed in the same lab[12]. These lab-developed tests (LDT) fall under separate regulations (CLIA certification) and are available if prescribed by a physician.[13]
Having an MCED test approved is a highly complex matter. It is governed by extensive and ever evolving legislation and regulations. Approval will depend on the context in which the MCED test is meant to be administered. For example, how is the test validated? Is it designed to be added to standard-of-care cancer screening modalities or to replace them? Is there a large enough average screening population that is eligible for MCED testing, such as the under-fifty demographic? What will be the economic impact and clinical outcomes of testing? And so on.
As for health insurance, there is no established evidentiary framework for payers to apply to a multi-cancer test assessment where the sensitivity of the test varies by cancer and by stage, and so the benefits and harms of screening will vary by tumor type.
Q: When will we know whether MCED tests have an impact on cancer detection, diagnosis and treatment outcomes?
AR: Further research[14] will be needed to assess which cancers are suitable for reducing mortality through regular MCED screening. Ideally, there should be prospective studies to evaluate MCED tests for their ability to identify cancers in individuals with previously undetected disease. Such studies take a long time, however. The alternative is randomized trials (screening vs. unscreened), and those will likely soon show a stage shift from advanced cancer to earlier cancer detection. It will also be necessary to understand the latent phase of the various cancers better (tumor behavior). The best observational studies compare mortality between screened and unscreened cancers over many years.
But even with MCED testing, it may still be years before there is any reduction in cancer mortality, which is particularly important for life insurers. Regulators, health insurers and cancer experts will likely play a critical role in helping to define new frameworks to advance these new technological approaches without waiting a decade or more for survival studies.
Q: When do you expect the first MCED tests to clear regulatory approval?
AR: My own personal view is that it is not unlikely MCED tests will be made available to the public early, i.e., perhaps within the next two years, and will be submitted to regulatory agencies for approval and reimbursement decisions long before trial results are available. As demand will likely be high, this may even start a new era of cancer screening, requiring extensive campaigns to educate both the public and the physicians whose job it will be to explain and prescribe these tests.
Tellingly, we have been in a similar situation before. Once the PSA test was approved for prostate cancer surveillance after diagnosis, PSA was swiftly applied for screening, too. Its impact on disease incidence, stage distributions, and – controversially – mortality was significant. But PSA screening rates were not tracked in real time and had to be compiled retrospectively for information on the link between PSA testing and changes in prostate cancer outcomes.[15]
Q: How will MCED testing impact the life insurance business?
AR: My own assessment is that in the medium term, MCED tests may have significant impacts on pricing assumptions, claims and underwriting for life insurance products. Critical illness (CI) policies will be the most impacted.
Depending on which cancers an MCED test will successfully screen for, pricing assumptions may need adjusting to reflect mortality improvements for cancers that are amenable to successful treatment.
In underwriting, we still have no satisfactory answers on how to assess individuals whose MCED test comes back positive without any clinical investigation to follow up with, or how to deal with applicants with a family history of cancer but a negative MCED test result. We may face a fair amount of adverse selection if MCED tests are offered without a prescription by a physician and positive results are not disclosed in applications for life or even CI insurance.
There may also be a debate on whether liquid biopsy should be equated to predictive genetic testing, which is subject to a legal ban in many markets. As I see it, however, MCED testing is anything but predictive. It merely detects and locates a mini cancer that is already present, and so should be unambiguously considered a diagnostic test.
Another challenge will be the basis on which cancer claims are eligible under CI policies. This will come into play once life insurers start defining eligibility not based on a definitive diagnosis by tissue biopsy, as they do today, but on a clear positive cancer signal obtained by a standardized MCED test. A further aspect of claims under CI policies, depending on claims definitions, would be earlier payouts. Ultimately, this will result in premiums being paid for shorter durations. In the era of MCED testing, moreover, indolent cancers that would never have been diagnosed before may now be eligible for CI claims.
So there a lot of contingencies where life insurance companies would do well not to rush ahead of the incremental growth in clinical knowledge. Having said that, the enthusiasm is palpable, and we are seeing start-up companies approaching reinsurers with new ideas in conjunction with MCED tests that they are offering.
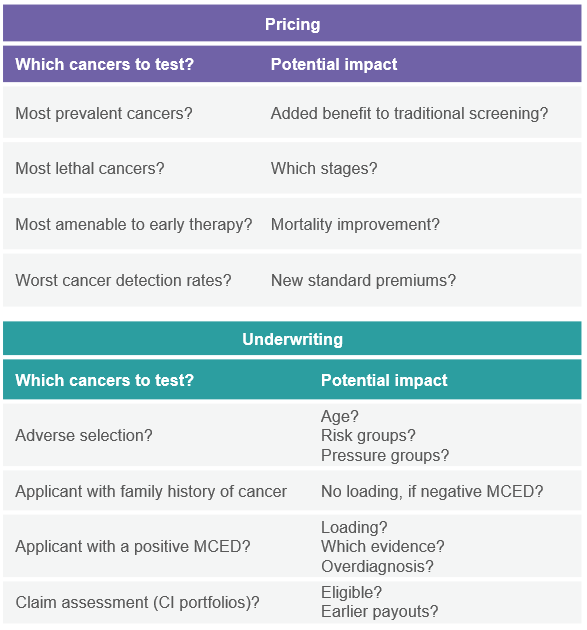
Aspects of potential impacts on Life business
Fig. 2 Questions to assess the impact on Life re/insurance business
Now, we have been talking about the many ways MCED testing may impact life insurance products. We also need to touch on health insurers. Indeed, they will have to tackle these challenges much earlier as they are the ones who will bear the brunt of spiraling add-on costs driven by diagnostic workups and treatments. Then again, in the medium term, MCED testing costs may be offset as early-stage detection leads to fewer advanced cancers, reducing the need for expensive therapies to treat them.
On balance, MCED tests represent an important advancement in cancer screening with a high potential for earlier treatment and mortality improvement. However, many questions described above still need to be addressed. PartnerRe continues to monitor these advances.
Contact PartnerRe
Our experts are always working on solutions for insurers to adapt their products to stay relevant and sustainable over the coming years. Do contact me if you would like to discuss this topic or to talk to one of our client partners about solutions for the new cancer detection reality.
Opinions expressed are solely those of the author. This article is for general information, education and discussion purposes only. It does not constitute legal or professional advice and does not necessarily reflect, in whole or in part, any corporate position, opinion or view of PartnerRe or its affiliates.