We believe you can go further and do more when you have a trusted risk-discussion partner on your team, who will look at your business holistically to uncover new opportunities.
We are a leading global reinsurer that helps insurance companies reduce their earnings volatility, strengthen their capital and grow their businesses through reinsurance solutions.
Diabetes management is advancing in many areas. One such area is the glucose control concept. Evidence suggests that HbA1C will no longer be the sole glucose control marker utilized in the management of this disease – an expanded approach with novel drugs and more frequent glucose monitoring is set to substantially improve diabetes mortality and morbidity risk.
Highlights
Cardiovascular complications are leading causes of mortality for diabetes.
The traditional approach to diabetes management – i.e., to managing hyperglycemia (an abnormally high blood glucose level) – is to focus on glucose control, primarily on the reduction of the HbA1C result (reflecting long-term, 2-3 month average glucose levels).
Past trials have, however, shown that well-controlled diabetes, measured by the HbA1C marker, does not consistently translate into the avoidance of adverse cardiovascular events. Furthermore, stringent glucose control via HbA1C can lead to increased cardiovascular mortality.1,9,18
Evidence continues to grow that in addition to the HbA1C level, the full, short-term glucose-level “wave-form” – including its peaks, troughs and rates of change – is also an important all-cause mortality and morbidity risk factor for diabetes.4,5
Recent novel drug trials reported a significant, previously unheard-of degree of reduction in cardiovascular and all-cause mortality risk for diabetes patients, adding weight to the need for a rethink of the traditional glucose control concept. It’s now considered that novel glucose-lowering drugs provide more stable glucose levels than past, glucose-lowering medications14 – and that this stability is in part responsible for the observed risk reduction.
The new dawn for optimal glucose control is therefore set to extend beyond the HbA1C, to include new tech (for continuous and shorter-term monitoring of glucose levels) and new drug classes to stabilize glucose levels.
HbA1C, a powerful marker for glucose control
The Hemoglobin A1C (HbA1C) blood test reflects and integrates an average of the mean blood glucose level from the past two to three months, thus providing a measure of “long-term glucose level”. This is the most used and recommended marker for glucose control. It has strong diagnostic and prognostic value for the development of diabetes complications (showing continuous, non-linear correlation with vascular and non-vascular mortality in diabetes)16,17 and is therefore extremely important for managing diabetes.
However, while HbA1C control has clear benefits for microvascular complications, there is a lack of definitive or consistent support for its value in reducing macrovascular complications.9,18
In fact, intensive glucose control has been associated with an increase in cardiovascular mortality.1 This is thought to be due to its most common side effect, hypoglycemia – defined as an abnormally low level of blood glucose caused unintentionally by medications given to lower the glucose levels of (hyperglycemic) diabetes patients. Hypoglycemia has multiple impacts. The best-known presentation is neuroglycopenia (including cognitive alteration, seizure and coma), but there are also less well known, but significant, vascular and cardiac complications driven by proinflammatory and electrophysiological effects, which can lead to progressive vascular changes and potentially to serious arrhythmias and sudden death.6,11,*
With the above caveats, HbA1C remains an important marker for diabetes management, but the current approach to optimal glucose control is now set to be significantly improved upon in a way that should substantially improve patient mortality and morbidity.
Glucose level (intra- and inter-day) fluctuations, the degree and speed of fluctuation and time spent within a desired glucose level range are now also being recognized as useful markers for diabetes management.
A concept in flux
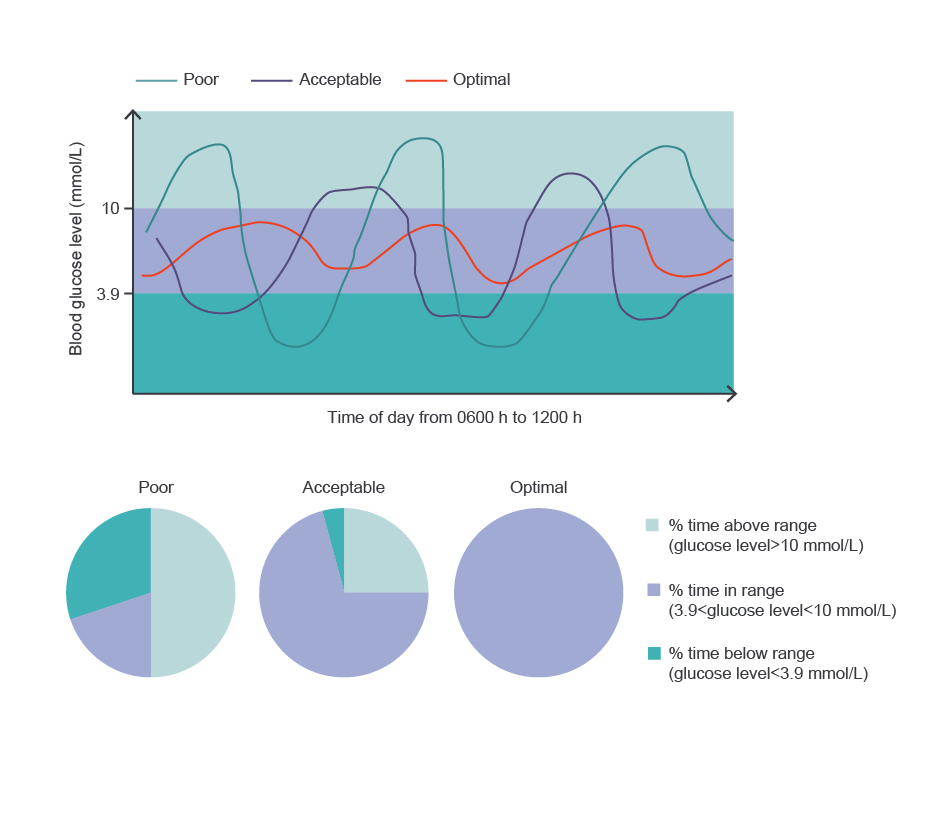
Individuals with the same HbA1C level can have widely varying intra- and inter-day glucose level fluctuations (figure 1).3
In recent novel drug trials, the novel glucose-lowering medications, the GIP1 analogs and SGLT2 inhibitors, demonstrated robust mortality reductions, though the overall benefit was not necessarily proportional in extent to improvements from HbA1C control.
These medications have since been observed to provide greater glucose level stability than previous glucose-lowering medications, suggesting that glucose level stability could be in part responsible for the mortality reduction.
There’s now growing evidence that it’s not just hyperglycaemia and hypoglycaemia, but also abnormal glucose variability and sudden shifts in glucose levels (with or without hypoglycaemia), that are detrimental to diabetes patients (see following section for more details).
Glucose level (intra- and inter-day) fluctuations, the degree and speed of fluctuation and time spent within a desired glucose level range are as a result now also being recognized as useful markers for diabetes management.
Abnormal glucose variability and sudden shifts
Abnormal glucose variability has now been found to be correlated with an increased risk of microvascular, cardiovascular complications and all-cause mortality.4,5,15 Glucose level stability is therefore a newly recognized factor for diabetes management – this requires that the glucose level stays within a target range (usually 3.9 to 10 mmol/L, apart from in special circumstances such as pregnancy), without sudden shifts within that range**, and for as long as possible.3 Abnormal glucose variability results if the criteria for glucose level stability are not met (and to various degrees).
Why no sudden shifts? It has been demonstrated4,11 that in addition to being caused by hypoglycemia, life threatening cardiac arrhythmias can also be caused by an upward or downward (with or without hypoglycemia, i.e., not necessarily reaching the levels that define hypoglycemia) sudden glucose level shift. A sudden oscillation in glucose level is a component of severe hypoglycemia because its treatment with oral or intravenous sugar is followed by a dramatic upward glucose level shift (iatrogenic).5,6
Time in range (TIR) is the proportion of time (for example, percentage hours per day) that a diabetic’s glucose level stays within the desired target range (see example in figure 1). The more time spent in TIR, the better.3
Figure 1: Three diabetes patients with identical HbA1C values (a long-term, 2-3 month average glucose control marker) display varying short-term (inter-day) fluctuations in glucose levels. The more time spent in the desired target range, here 3.9-10 mmol/L, known as “Time in Range (TIR)”, the lower the patient’s mortality and morbidity risk. Source: Ceriello (2022).3
New tech, the perfect partner
Glucose levels can be monitored on a short or longer-term (in which case HbA1C testing is ideal) basis. Short-term monitoring refers to intra-day levels (measured ‘at any time’, including via fasting glucose level and 1- and 2-hour postprandial glucose levels tests) or inter-day glucose levels (how these intra-day measures move day by day).
Advanced technology enabling frequent or continuous glucose monitoring therefore has great benefit here, capturing the full, short-term wave form of glucose levels.20 Availability/accessibility remains limited, but as this widens, patient outcomes will improve.
A new dawn for diabetes management – based on the full glucose wave form
The new findings indicate that it’s not just long-term glucose levels (monitoring via HbA1C) that matter for diabetes management, but also, in order to reduce the risk of adverse cardiovascular events and all-cause mortality, how the glucose level moves over a much shorter time-frame – including how often it moves out of the target range and whether sudden shifts take place.
Therefore, to improve diabetes mortality and morbidity, the aim of glucose control is now to move beyond reaching and maintaining optimal HbA1C values, to also achieving more stable desired long- and short-term glucose levels via novel glucose-lowering drugs and the more frequent monitoring of glucose levels i.e. via new tech.
Please contact us if you would like to find out more about this development for diabetes management and/or to discuss the mortality and morbidity impacts or new product initiatives. We would be happy to set up a meeting with you.
Contributor
Dr. Emoke Posan, Chief Medical Officer, North America
Opinions expressed herein are solely those of the authors. This article is for general information, education and discussion purposes only. It does not constitute legal or professional advice and does not necessarily reflect, in whole or in part, any corporate position, opinion, endorsement or view of PartnerRe or its affiliates.
Footnotes
*: Progressive retinopathy is also a well-known complication of recurrent hypoglycemia (Dandona). Hypoglycemia is proarrhythmic: can cause sudden epinephrine release with sudden electrophysiological changes, heterogeneity in repolarization, QT prolongation leading to various arrhythmias, atrial fibrillation, ventricular arrhythmias and sudden cardiac arrest.
**: A sudden downward shift within or below the target range is not necessarily indicative of hypoglycemia (defined as abnormally low levels of blood glucose).
References
The ACCORD study group. Long-Term Effects of Intensive Glucose Lowering on Cardiovascular Outcomes. N Engl J Med 2011; 364:818-828. DOI: 10.1056/NEJMoa1006524
Begic E. et al. Diabetes: total risk – benefit of SGLT2 inhibitors and GLP1 agonists. ESC e-Journal of Cardiology Practice Volume 22 2022 v 22, N° 9 – 20 Apr 2022. https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-22/diabetes-total-risk-benefit-of-sglt2-inhibitors-and-glp1-
Antonio Ceriello; Glucose Variability and Diabetic Complications: Is It Time to Treat? Diabetes Care 1 June 2020; 43 (6): 1169–1171. https://doi.org/10.2337/dci20-0012
Ceriello A et al. Glycaemic variability in diabetes: clinical and therapeutic implications. Lancet Diabetes Endocrinol 2019;7: 221–230. doi: 10.1016/S2213-8587(18)30136-0
Chow, Elaine, et al. “Risk of cardiac arrhythmias during hypoglycemia in patients with type 2 diabetes and cardiovascular risk.” Diabetes5 (2014): 1738-1747.
Comprehensive Management of Cardiovascular Risk Factors for Adults With Type 2 Diabetes: AScientific Statement From the American Heart Association Circulation. 2022;145:e722–e759. DOI: 10.1161/CIR.0000000000001040
Diabetes Control and Complications Trial (DCCT): results of feasibility study. The DCCT Research Group. Diabetes Care. 1987 Jan-Feb;10(1):1-19. doi: 10.2337/diacare.10.1.1
ESC e-Journal of Cardiology Practice Volume 22 2022 vol. 22, N° 9 – 20 Apr 2022.
Diabetes Canada. Chapters 9 and 13. http//guidelines.diabetes.ca/cpg.
Guideline Standards of Medical Care in Diabetes; American Diabetes Association. Clin Diabetes2022;40(1):10–38. https://org/10.2337/cd22-as01
Lee H et al. Glycemic Variability Impacted by SGLT2 Inhibitors and GLP 1 Agonists in Patients with Diabetes Mellitus: A Systematic Review and Meta-Analysis. J Clin Med. 2021 Sep 9;10(18):4078. doi: 10.3390/jcm10184078
Li, Diabetes Care. Visit-to-Visit HbA 1cVariability Is Associated With Cardiovascular Disease and Microvascular Complications in Patients With Newly Diagnosed Type 2 Diabetes. 2020 Feb;43(2):426-432. doi: 10.2337/dc19-0823. Epub 2019 Nov 14
Raghavan S et al. Diabetes Mellitus-Related All-Cause and Cardiovascular Mortality in a National Cohort of Adults. J Am Heart Assoc. 2019 Feb 19;8(4):e011295. doi: 10.1161/JAHA.118.011295
Holman R.R et al. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. Engl J Med 2008; 359:1577-1589. DOI: 10.1056/NEJMoa0806470
Zinman et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015 Nov 26;373(22):2117-28. DOI: 1056/NEJMoa1504720