We believe you can go further and do more when you have a trusted risk-discussion partner on your team, who will look at your business holistically to uncover new opportunities.
We are a leading global reinsurer that helps insurance companies reduce their earnings volatility, strengthen their capital and grow their businesses through reinsurance solutions.
Global prevalence continues to increase; this is now the fastest growing patient group. Diabetics are usually not considered a good Life risk. Most underwriting guidelines are restrictive. Many living benefit insurance applications are declined.
That’s the bad news. Now for the good news.
Two significant and parallel change factors – innovative new medicines and advances in digital technologies – are shifting diabetes management into a new and more positive era, significantly improving the prognosis and quality of life for diabetics, and paving the way for new Life underwriting and product opportunities.
Increasing global prevalence
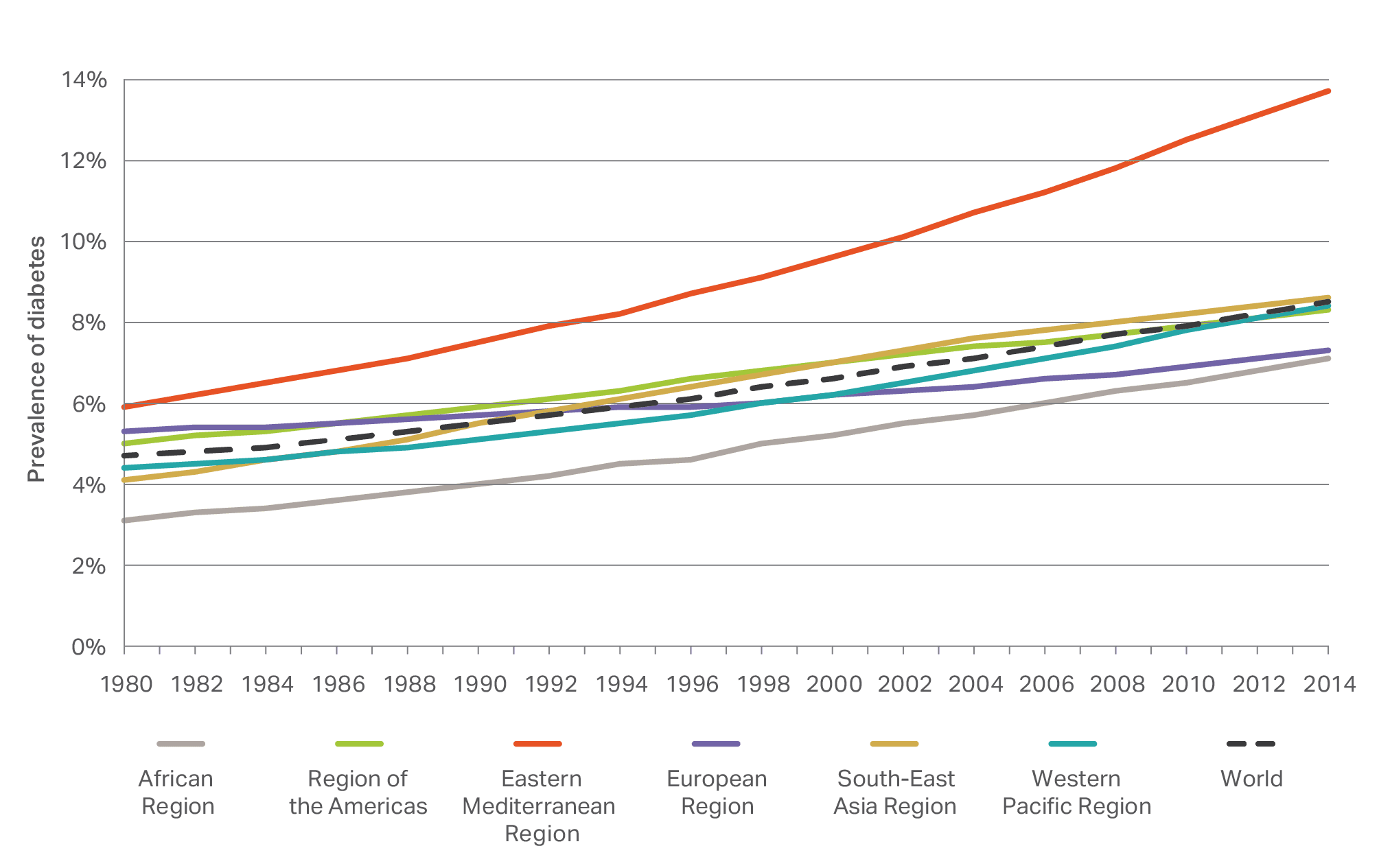
Diabetes is a major and ongoing societal issue. The global prevalence of diabetes increased from 4.7% in 1980 to 8.5% in 20141 (figure 1); and that’s not including ‘silent diabetics’, the estimated 2-3% of the population whose diabetes has not yet been diagnosed2. Prevalence has increased alongside obesity prevalence in almost all countries during this period2, rising faster in low- and middle-income countries than in high-income countries1.
Figure 1: Global prevalence of diabetes, 1980 to 2014, by region and combined. Source: WHO1.
Higher mortality
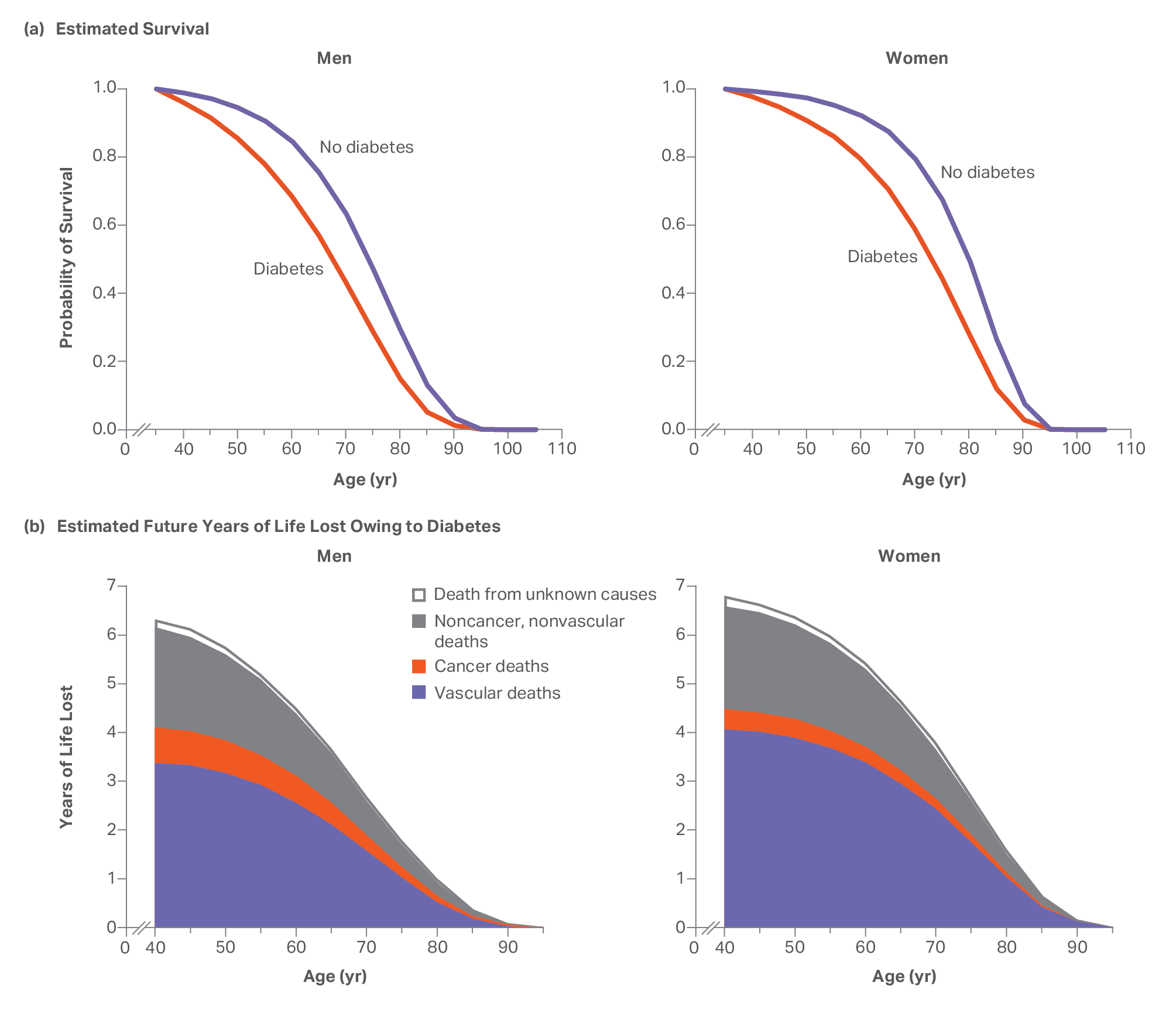
As shown in figure 2, diabetes leads to a higher mortality for men and women, at adult ages3. Translating this into years of life lost, a 50-year old male with diabetes has, on average, a six year reduced life expectancy compared to those without diabetes (for smoking it would be ten years). Cause of death is predominantly vascular, i.e. heart attacks and strokes as a result of plaques forming within arteries (premature atherosclerosis).
Figure 2: (a) Estimated survival curves for men and women with and without diabetes, and (b) corresponding estimated years of life lost due to diabetes by cause of death. Data from multiple, mainly high-income countries. Source: NEJM3.
But mortality and ‘complication-related morbidity’ rates are improving
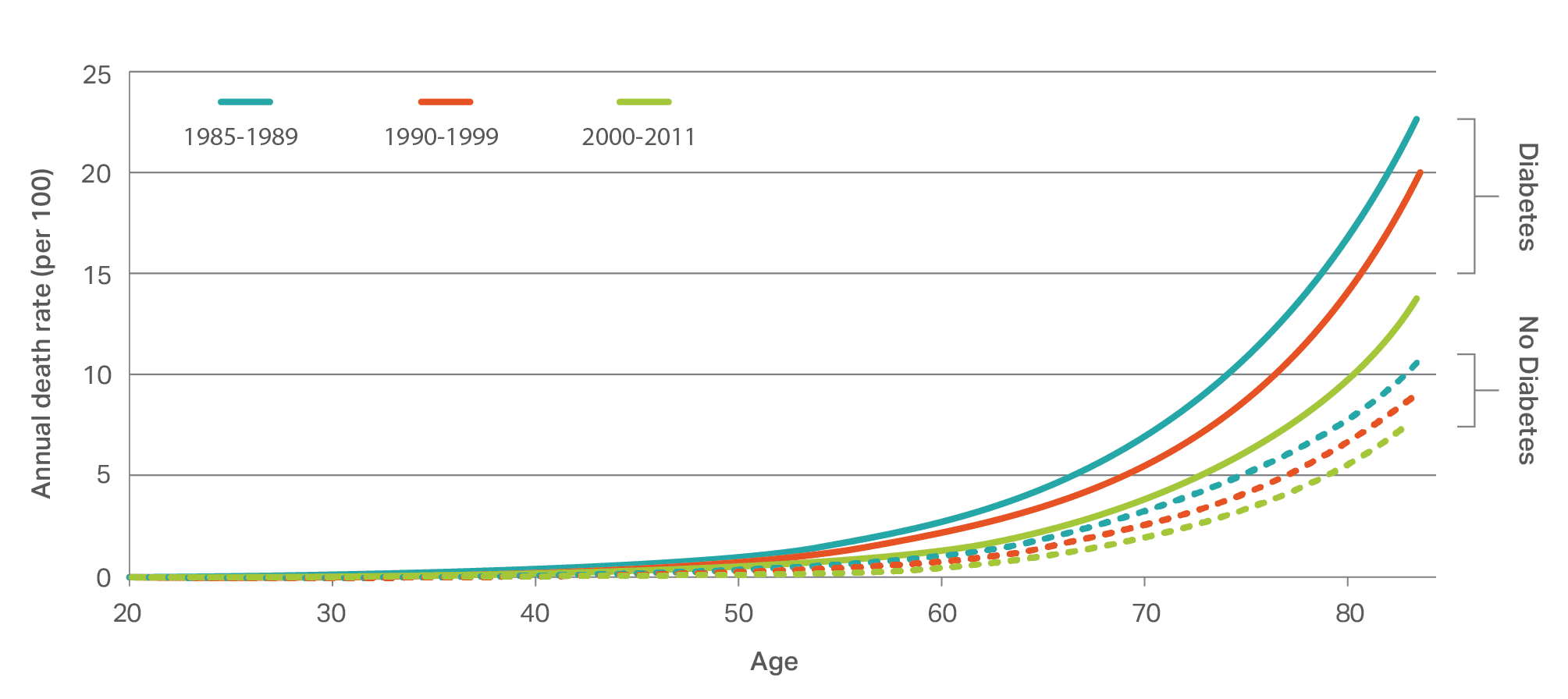
Despite higher mortality rates for diabetics compared to non-diabetics, the mortality (data mainly from high-income countries) of diabetics is steadily improving (figure 3 and figure 4). For example, all-cause mortality rates for type 2 diabetics improved by 15-40% every 10 years between 1995 and 20134.
Incidence rates for developing diabetes complications (morbidities) are also improving: in the US between 1990 and 2010, for example, diabetes linked heart attacks fell by 68%, strokes by 53% and amputations by 52%5. Over a similar period, retinopathy and blindness fell by 40-50% in Israel and Southern Germany4.
Figure 3: Annual all-cause death rate among men, US, by age, for diabetics and non-diabetics during the specified three time periods. There is a clear improvement for diabetics over time which exceeds that of the non-diabetic populations. A similar result was noted for females. Source: Gregg et al.6.
Figure 4: Trends in rates of all-cause mortality among populations with diagnosed type 2 diabetes. The data shows ongoing mortality improvement in the countries shown. Source: Gregg et al.4.
“We are working in partnership with insurers to develop innovative Life insurance solutions for diabetics.”
An even brighter future
The focus of diabetes treatment/management has been to control blood sugar levels with sulfonylureas (metformin) or insulin and diet, delivering the positive trends outlined above.
Several significant recent change factors – spanning conventional medical advances and digital technological breakthroughs – are set to accelerate the trend. Indeed some are already taking effect:
A wider multifactorial approach that adds concomitant risk factors, such as elevated blood pressure or lipids, to the diabetes management toolbox.
Innovative drugs with new mechanisms, such as SGLT2 inhibitors and GLP-1 receptor antagonists, have come onto the market to treat diabetes; many new drugs are under development. Several studies have found these to be particularly cardio-protective; initial studies indicated mortality reductions (fewer heart attacks) within the first few years7.
Plus new diabetes classification to boost potential for personalized medicine
Tailoring treatment to the individual characteristics of each diabetes patient may soon be taken to a new level by the latest research into the heterogeneity of the disease.
Several Scandinavian studies8 have indicated that diabetes is more heterogeneous than type 1 and type 2 (table 1). These studies identify five diabetes ‘clusters’ (table 2). The expectation is that this could soon open up new possibilities for more targeted diabetes monitoring and therapy. For example, cluster 3 individuals, having a significantly higher risk of diabetic kidney disease, may be checked for this progression more closely than cluster 4 individuals. These preliminary categories still need to be corroborated by larger population studies, but the early indications are promising.
Type 1
Type 2
Age
Mostly children
Adults
Manifestation
Sudden
Gradual
Proportion
5%
90%
Cause
Autoimmune
Genetics, obesity, lifestyle
Mechanism
Insulin deficiency
Insulin resistance
Treatment
Insulin
Diet, Metformin, Insulin
Table 1: Current classification of diabetes into type 1 and type 2 diabetes9. This division impacts treatment programs. Source: Compiled by PartnerRe.
Insulin treatment typically necessary in the first instance
2
Type 2
Insulin-deficient diabetes (SIDD)
Similar to cluster 1
High HbA1c
Low insulin secretion
GADA-negative
Highest incidence of early retinopathy
Insulin treatment often necessary but considerable time required to reach treatment goal (HbA1c <52 mmol/mol)
3
Type 2
Insulin-resistant diabetes (SIRD)
Relatively low HbA1c
Insulin resistant
Persistent macroalbuminuria
Highest incidence of nephropathy (kidney)
Highest prevalence of non-alcoholic fatty liver disease
Insulin treatment often not necessary
4
Type 2
Obesity-related diabetes (MOD)
Not insulin resistant
Insulin treatment often not necessary
‘Healthier’ obesity?
5
Type 2
Age-related diabetes (MARD)
Similar to cluster 4
Modest metabolic alterations
Insulin treatment often not necessary
Table 2: The current two categories of diabetes (type 1 and type 2)9 are potentially set to evolve into five categories. This stands to significantly improve treatment programs for diabetics; effectively enabling a more ‘personalized medicine’ approach for treating and managing diabetes. Source: Compiled by PartnerRe.
Plus powerful new tech – Wearables and AI are key
Technological advances are poised to take diabetes mortality and complication-related morbidity improvements to another level.
Until recently, most diabetics checked their blood glucose by intermittent finger-prick testing four to eight times a day. Change is already underway. Modern digital technology with subcutaneous sensors has evolved dramatically over recent years and is now offering diabetics new possibilities to monitor their glucose profiles more conveniently and without the pain and blood of finger-prick testing.
Two types of digital glucose monitoring systems are currently available: real-time continuous glucose monitoring (CGM) and flash glucose monitoring (FGM). CGM technology is currently only used for type 1 diabetes and is more reliable than FGM, which is used for type 1 and 2 diabetes and measures glucose levels only on demand.
Both monitoring systems can be seen as an intermediate step toward an open loop system that may eventually replace the diseased pancreas (see below, ‘The next step – an artificial pancreas?’).
A huge, imminent step forward is the integration of these technologies with artificial intelligence, as recently approved by the FDA for Medtronic’s Guardian Connect CGM system based on IBM Watson technology. The artificial intelligence element of this system enables prediction of glucose levels with a very high level of accuracy by comparing the patient`s data with that of diabetics with similar glucose profiles.
The next step – an artificial pancreas?
With these new technological capabilities, tremendous strides are being made in research to develop an artificial pancreas device system that automatically monitors glucose levels and adjusts insulin dosage also according to nutrition and lifestyle.
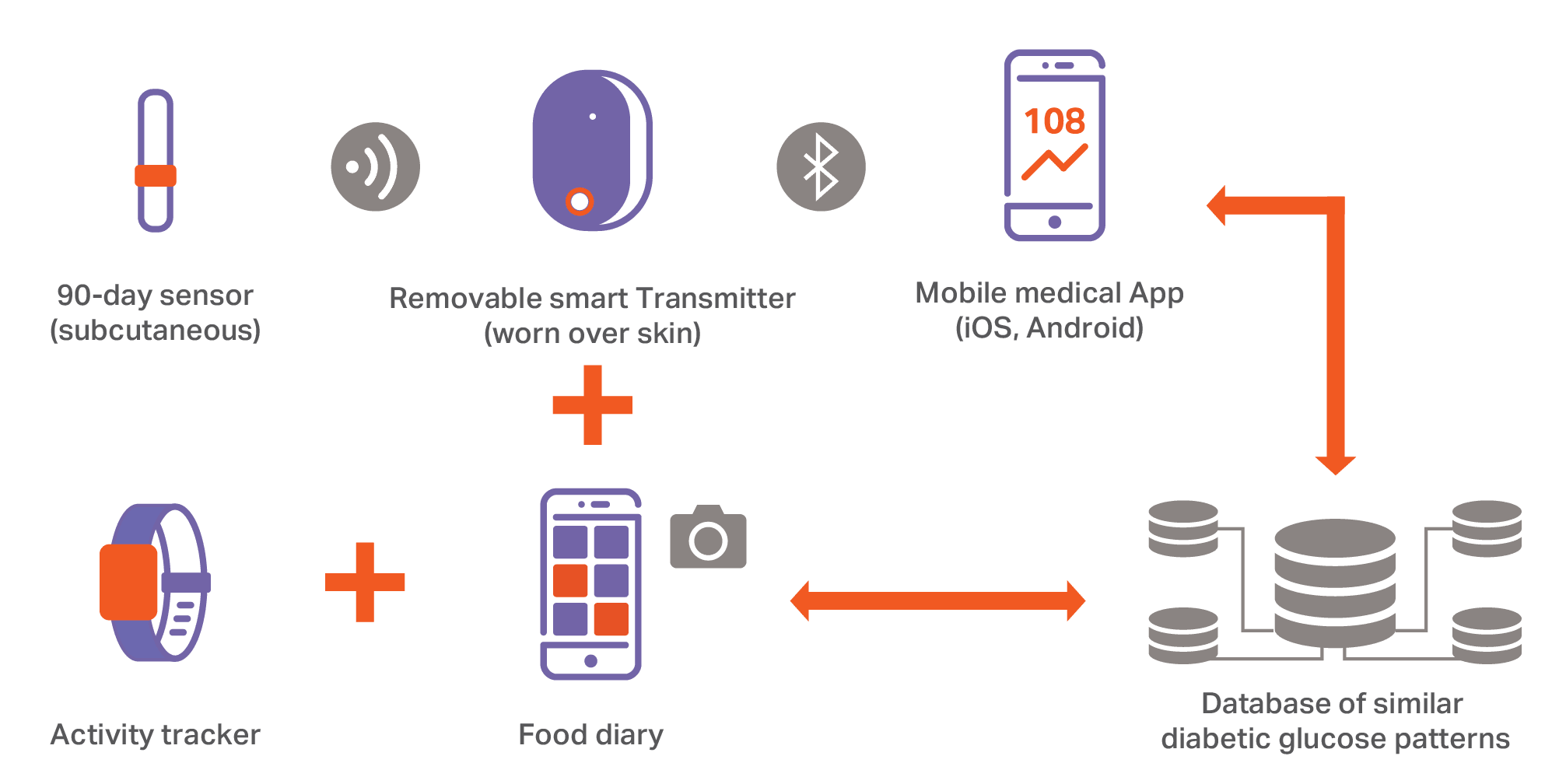
So in the near future, alongside the traditional medical world, the expectation is that there will also be a digital world (figure 5) consisting of a sensor, transmitter, insulin pump, smartphone app and a wearable or wrist watch measuring physical and other vital signs – all combined with comprehensive cloud-based databases of other diabetic individuals and processed by artificial intelligence.
Figure 5: Diabetes management by artificial intelligence. Illustrative example of what the future could hold; an artificial, completely digital pancreas. Envisaged is an open loop system comprising sensors and wearables, smartphones and cameras, connected devices, telemedicine, cloud technology and cognitive AI. Source: PartnerRe.
Business implications for Life & Health insurance
As described, diabetes mortality and complication-related morbidity will be substantially reduced by improved metabolic controls and treatments.
At the same time, the increased usage of digital technology will provide underwriters (within the framework of data regulation and the insured’s agreement) with substantial volumes of data for substandard lives underwriting.
Underwriting. Initially, life products are likely to benefit from data indicating reduced mortality risk, while underwriting change implementation for morbidity products, such as disability covers and critical illness, typically requires caution through the medium term until sufficient experience is available.
Product development. Continuous underwriting models are already feasible, involving regular interaction with the insured and, for example, integrated links to wellness programs and coaching for a healthier lifestyle. With the advances detailed in this paper, opportunities arise to derive innovative, dynamically underwritten products for diabetics. Reinsurance partners can help in this respect. An illustrative example of reporting options for continuous underwriting for diabetics is shown in table 3.
Sales & marketing. These changes indicate a positive sales outlook: Premiums are likely to become more attractive for diabetics and cases that would previously have been declined are more likely to be accepted, with or without restrictions, e.g. loadings or stepwise coverage extensions.
Activity tracking through wearable (moderate discount @ fixed point)
7-10%
Submission of blood reports-HbA1c level (higher discount @ fixed point)
15-20%
Highest discount linked to CGM (AI linked, real-time & dynamic)
Up to 50%
Table 3: Illustrative example of reporting options for continuous Life products enabled by the imminent, new tech tool kit for diabetes management. Premium discounts are solely for visualization. Source: PartnerRe.
Of course, as with any living Life & Health product, these trends must be monitored alongside the negative trends in global diabetes incidence rates and the obesity pandemic.
New era, new opportunity
From an era of declination and high premiums – and for a patient group that increasingly does not consider itself to be ill – these combined developments stand to bring us into a new era of acceptance, improved risk management and new, innovative insurance products. These changes will likely apply initially only in high-income countries, but will hopefully be taken up more widely as losses fall and the benefits are better understood.
In all, these positive developments offer diabetics a brighter future and represent a unique opportunity for Life & Health insurers to become more relevant and connected to their insureds.
Your reinsurance partner for developing a new generation of insurance products for diabetics
Our Life & Health teams are closely monitoring all these advances and we will accordingly adjust our PAR medical underwriting manual at the appropriate times.
The PAR (Partner in the Assessment of Risk) Medical Underwriting Manual
Available to all PartnerRe Life clients
Make fast, operationally efficient, knowledge-based underwriting decisions for all Life insurance products
Risk-based loadings for substandard lives
Coming soon: PAR V2:0
We are currently working with our clients and regional partners to deliver new, innovative product solutions for diabetics.
If you are interested in a partnership to trial and develop these products with us, please get in touch, we look forward to hearing from you!
Contributor
Dr. Achim Regenauer, Chief Medical Officer, PartnerRe
This article is for general information, education and discussion purposes only. It does not constitute legal or professional advice of PartnerRe or its affiliates.