We believe you can go further and do more when you have a trusted risk-discussion partner on your team, who will look at your business holistically to uncover new opportunities.
We are a leading global reinsurer that helps insurance companies reduce their earnings volatility, strengthen their capital and grow their businesses through reinsurance solutions.
As and when the pandemic becomes endemic, will the waters calm and mortality soon return to its pre-pandemic levels and patterns? Our experts show – with the help of a simple modeled example of the ongoing impact of delayed cancer diagnoses and treatments – why “secondary” excess mortality and mortality assumption uncertainty is in fact likely to continue for several more years.
The excess total mortality observed to accompany the pandemic’s waves through 2021 is globally well documented (see US example in figure 1).
Figure 1: US deaths per week, 2021 (all causes) for the age group 45-64, against the 2017-2019 average number of deaths. The excess mortality (orange shaded area) follows Covid’s waves. Data source: CDC.1
But what can we expect as (assumingly) the pandemic subsides and becomes endemic? Will pre-pandemic total mortality and cause of death percentages – led by non-communicable diseases such as heart attacks, stroke and cancer – bounce back in 2022 to their pre-pandemic levels and confidence quickly return to the setting of mortality assumptions?
Unfortunately, it’s not that simple because of several indirect drivers which could contribute to a secondary post-pandemic excess mortality – primarily, see figure 2, from cancer (delayed cancer treatments and diagnoses leading to more later-stage cancers), cardiovascular disease (triggered by thrombotic vasculitis due to SARs-CoV-2 infection), mental/neurologic/psychological disease (e.g., from lock-down impacts), lifestyle (increased obesity) and Long Covid.
Figure 2: Schematic diagram showing a simplified subgrouping of drivers that could contribute to a post-pandemic, secondary excess mortality. Cancer, in our view, will likely have the highest impact on excess mortality and is the focus of this article. Long Covid is known as a morbidity risk, but there are now indications of it also being a mortality risk. Source: PartnerRe.
These indirect excess mortality drivers have the potential to maintain the energy of Covid’s “mortality ripples” even once the pandemic has become endemic, and to challenge the setting of mortality assumptions for years to come.
Example: Long Covid as a post-Covid excess mortality driver
Long Covid is primarily known as a morbidity risk and is associated with a range of symptoms.2 However, several studies, have now additionally identified Long Covid as a mortality risk for previously hospitalized Covid patients, i.e., after the acute hospitalization episode. For example, a US cohort study3 found that for the cohort and after adjustment for comorbidities, age, gender and ethnicity, leaving Covid as the sole variable, the likelihood of dying within 12 months of a positive test was found to be two to three times higher for previously hospitalized patients with moderate and severe Covid. Cohort patients with mild Covid experienced no increase in mortality at 12 months.
Even minor shifts to higher-stage breast cancers at diagnosis will have a significant and ongoing impact on mortality.”
Example: Cancer as a post-Covid excess mortality driver
In our view, cancer is likely to be the main contributor to Covid’s secondary excess mortality. Covid lockdowns and massive strains on healthcare facilities led to missed and delayed cancer screenings, appointments, treatments and surgical removals of cancer. In the US, for example, over 8 million less mammograms (-21%) were carried out in 2020 c.f. 2019, equating to approximately 41,500 delayed individual breast cancer diagnoses4 (fewer Critical Illness insurance claims can as a result be expected, a trend that we have observed in our markets). This screening reduction/delay matters as it means that more breast cancers will be diagnosed at later cancer stages (pre-Covid, the majority of breast cancers were screened and diagnosed at early stages5, with a high chance of successful treatment). Later-stage cancers are treated less efficiently, have lower survival rates (see also figure 3b) and require increasingly expensive drugs. More later-stage cancers will therefore lead to higher mortality.
This indirect excess mortality driver is all the more important to monitor because it is not a short-term blip – reduced routine screening rates around the world continue to this day, a situation compounded by ongoing healthcare waiting list bottlenecks.6
To what extent could a shift to later-stage cancers impact mortality – a simple model
To assess the potential impact on mortality of a plausible shift to later-stage cancers from delayed screening alone, we carried out a simple model analysis (see below, figures 3, 4 and 5).
The base data for the analysis was the 2019 pre-Covid distribution of US SEER breast cancer stages at diagnosis (figure 3, “Base”) and corresponding 1-, 3- and 5-year cumulative mortality rates for each stage (figure 4).7,8 Later stages have notably higher cumulative mortality rates, indicating that even minor shifts to later-stage breast cancers at diagnosis will have a significant (and ongoing) impact on mortality.
To the base, pre-Covid data, we applied three reasonable pandemic stress scenarios of increasing impact, and for each calculated the distribution of cancer stages at diagnosis. The stresses are expressed as progressive shifts to later-stage cancers at diagnosis (figure 3, “Stresses I-III”). Given publicly available information, we consider scenario “Stress II” as neither overly optimistic nor overly conservative, and therefore set it as our central stress scenario.
Figure 3: Comparison of the pre-Covid 2019 (base) distribution of US breast cancer SEER stages at diagnosis against three healthcare stress scenarios (stress I-III) of increasing severity. The majority of the pre-Covid base breast cancers were diagnosed at early (localized and regional) stages. The three stress scenarios exhibit a progressive shift to later-stage cancers at diagnosis (associated, as shown in figure 4, with lower survival rates). Source: SEER7 and the American Cancer Society8 (data); PartnerRe (model analysis).
Figure 4: Pre-Covid, base (in this case 2009-2013) cumulative mortality rates by SEER stage at diagnosis, showing the notably higher mortality of breast cancers diagnosed at later stages. Source: SEER7 and the American Cancer Society8 (data); PartnerRe (model analysis).
To evaluate the approximate mortality impact over time, assuming a simplified one-year (2020) healthcare disruption, we then modeled the mortality impact over time (up to 5 years after diagnosis) for a single cohort of newly diagnosed patients for the base and stress scenarios (figure 5). Based on this simplified model of one cancer type, one disruption year and crudely isolating the impact of delayed cancer screening only, we observed notable increased mortality even at 5 years after diagnosis.
Figure 5: Mortality impact to a cohort of newly diagnosed patients after a single disruption year (2020). Mortality is above the base level even 4-5 years after diagnosis. Source: SEER7 and the American Cancer Society8 (data); PartnerRe (model analysis).
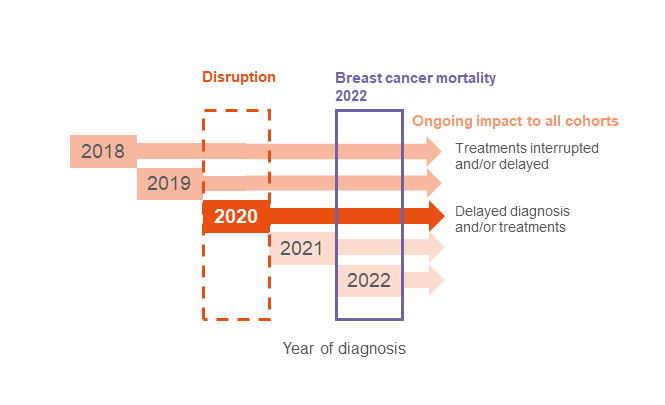
To indicate the potential impact to an insurance portfolio, we then included in the model several earlier pre-Covid diagnosis year cohorts whose treatments would have been delayed and treatment backlog disruption assumptions for 2021 and 2022 (figure 6). This aggregated ‘portfolio’ cohort view indicated a breast cancer mortality increase for 2022 of up to 10%. Although crudely done, this level of increase and the prolonged medium-term outlook is supported by a recent Canadian model-based study.9
Figure 6: 2022 breast cancer mortality cohort composition – an insurance portfolio visualization of the impact of a single year (2020) pandemic disruption on multiple year cohorts. Previous (2018 and 2019) diagnosed cohorts are affected by interrupted and/or delayed treatments. The 2020 cohort suffers from delayed diagnosis and treatments and is likely to be the most affected (see impacts over time in figure 5). Later cohorts (2021, 2022 and beyond) may also suffer from delayed diagnosis and treatments due to ongoing backlogs in the healthcare system. Source: PartnerRe.
To obtain a more complete view of cancer’s indirect excess mortality impacts, other cancer types, geographical variations, more granular age bands and compounding disruption years would also need to be modeled, together with applying multiple uncertainty estimations to the disruption scenarios themselves (e.g., relating to the number and duration of future Covid waves, the resilience of healthcare systems and peoples’ behaviors). The majority of these, however, are likely to further increase the excess mortality. For an even fuller picture, the impacts of Covid’s other indirect mortality drivers (figure 2) would also need to be modeled, and population data be adjusted to reflect an (on average healthier) insured population.
Ongoing pandemic mortality assumption uncertainty
We progress now through a phase of post-pandemic mortality uncertainty. The above analysis supports the hypothesis that a significant, secondary excess mortality will persist beyond 2022, impacting both new and in-force Life insurance business. For breast cancer alone, for example, a portfolio-view excess mortality of up to 10% for 2022 has been estimated. Other above-mentioned drivers will additionally need to be taken into account and years beyond 2022 will also be impacted. Continuing to regularly review pandemic mortality assumptions over the coming years is therefore recommended.
Contributors:
Achim Regenauer, Chief Medical Officer, Europe and Asia Pacific Florian Gomez, Head of Risk Modelling
Opinions expressed herein are solely those of the authors. This article is for general information, education and discussion purposes only. It does not constitute legal or professional advice and does not necessarily reflect, in whole or in part, any corporate position, opinion, endorsement or view of PartnerRe or its affiliates. Additionally, we must stress that there is, as always, considerable uncertainty involved in discussing future risk drivers and trends, and that the scenarios and numerical calculations set forth herein are simplified and for illustrative purposes only.
3 Mainous III AG, Rooks BJ, Wu V and Orlando FA (2021) COVID-19 Post-acute Sequelae Among Adults: 12 Month Mortality Risk. Front. Med. 8:778434. https://doi.org/10.3389/fmed.2021.778434
7 US National Cancer Institute Surveillance, Epidemiology and End Results (SEER) program; https://seer.cancer.gov/explorer/ SEER*Explorer Application (cancer.gov)
8 American Cancer Society; https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2019-2020.pdf Breast Cancer Facts & Figures 2019-2020
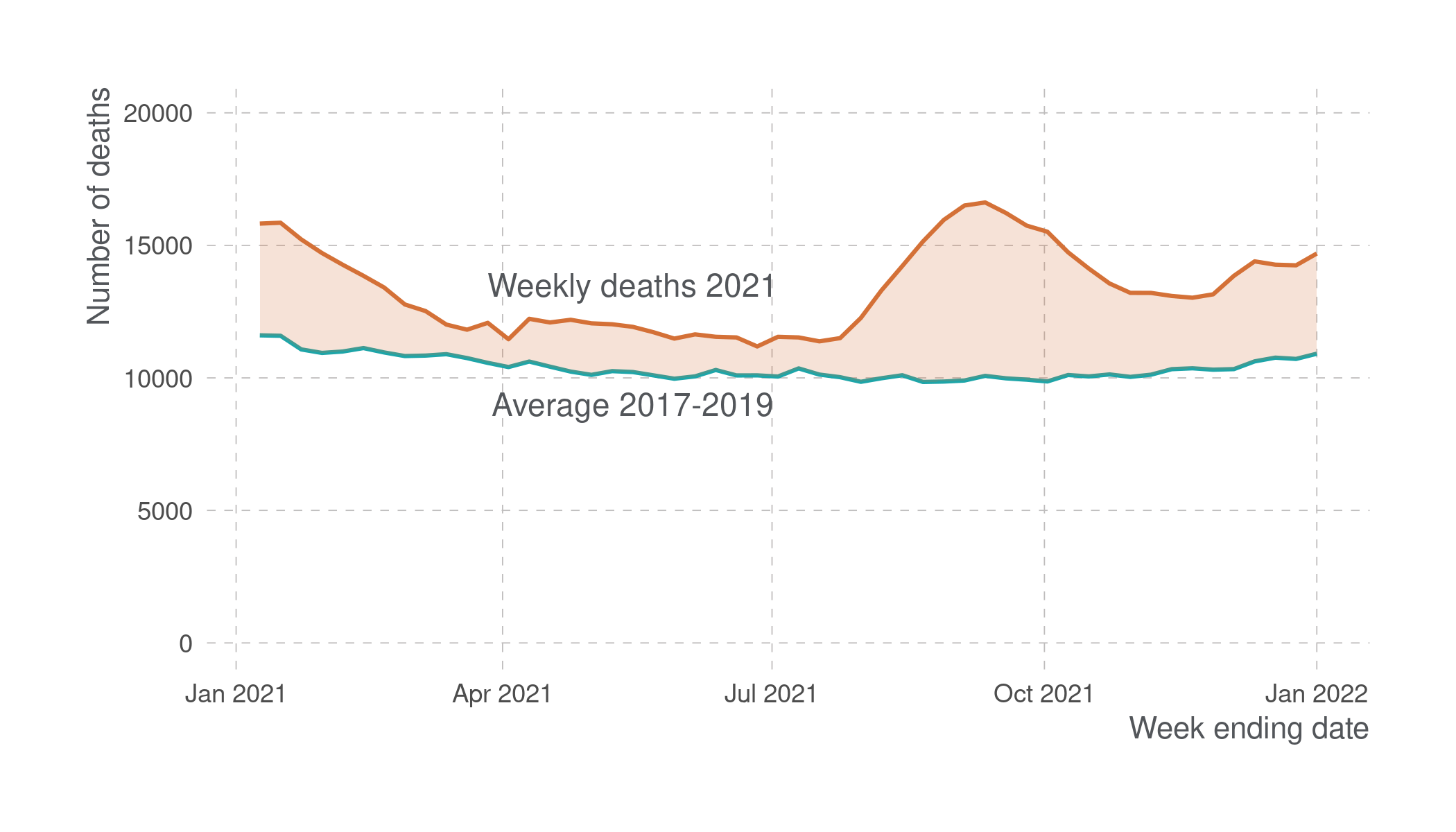 Figure 1: US deaths per week, 2021 (all causes) for the age group 45-64, against the 2017-2019 average number of deaths. The excess mortality (orange shaded area) follows Covid’s waves. Data source: CDC.1
Figure 1: US deaths per week, 2021 (all causes) for the age group 45-64, against the 2017-2019 average number of deaths. The excess mortality (orange shaded area) follows Covid’s waves. Data source: CDC.1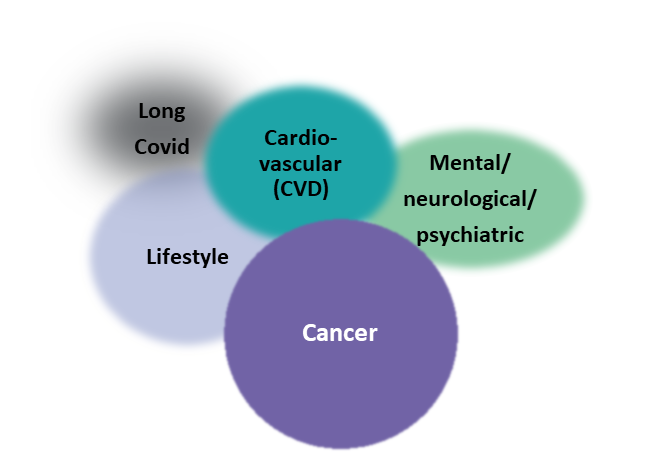
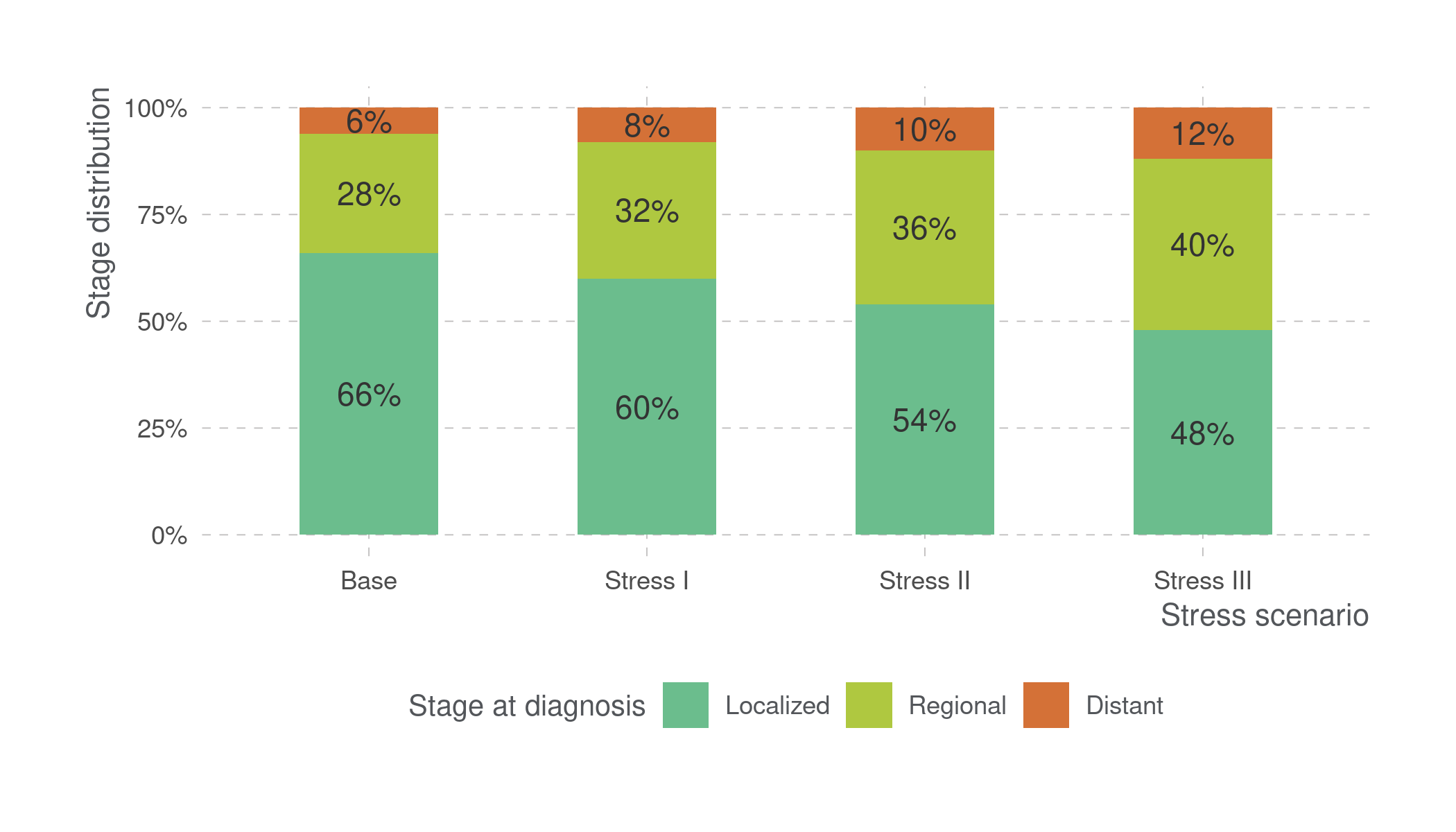
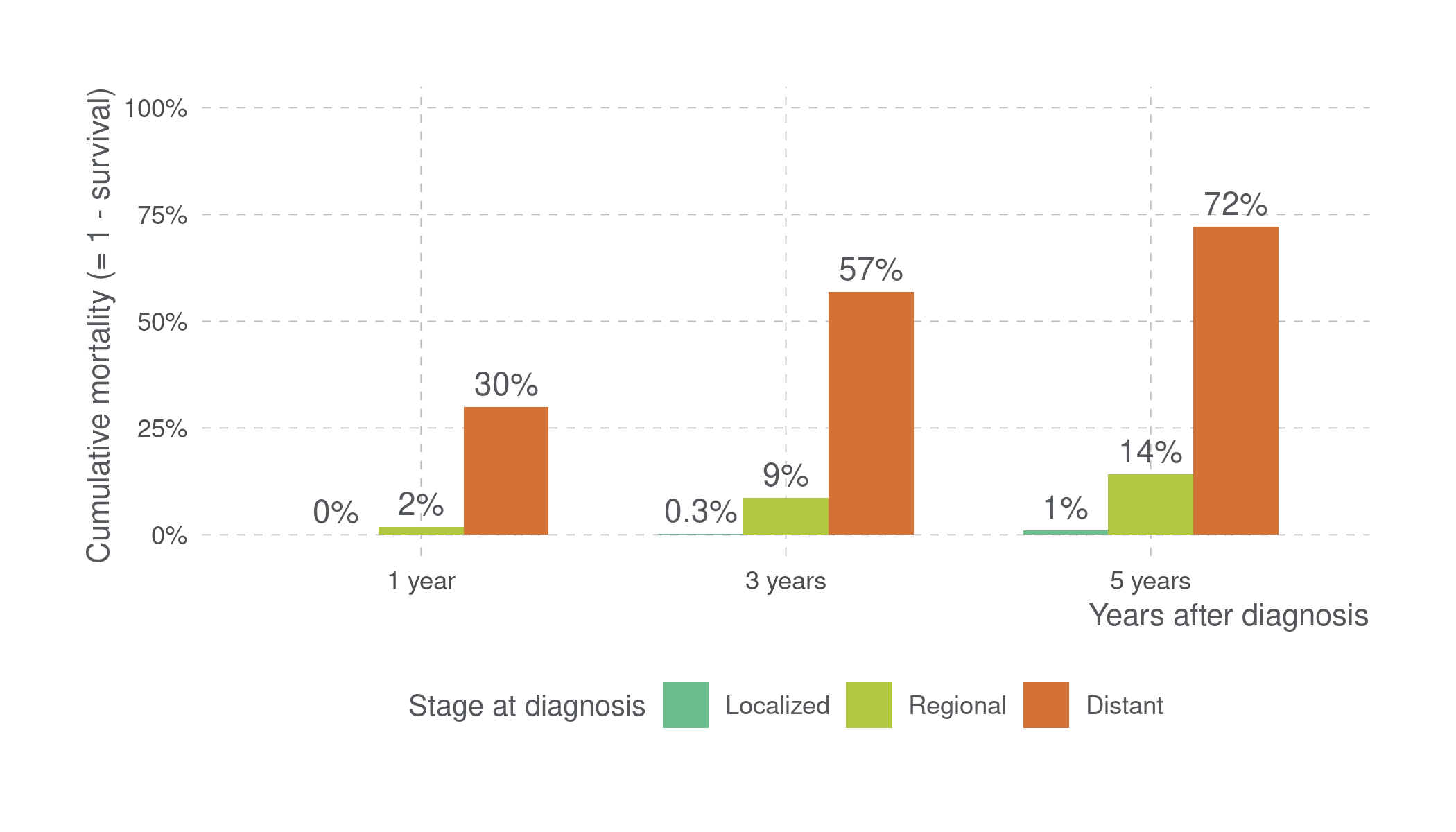 Figure 4: Pre-Covid, base (in this case 2009-2013) cumulative mortality rates by SEER stage at diagnosis, showing the notably higher mortality of breast cancers diagnosed at later stages. Source: SEER7 and the American Cancer Society8 (data); PartnerRe (model analysis).
Figure 4: Pre-Covid, base (in this case 2009-2013) cumulative mortality rates by SEER stage at diagnosis, showing the notably higher mortality of breast cancers diagnosed at later stages. Source: SEER7 and the American Cancer Society8 (data); PartnerRe (model analysis).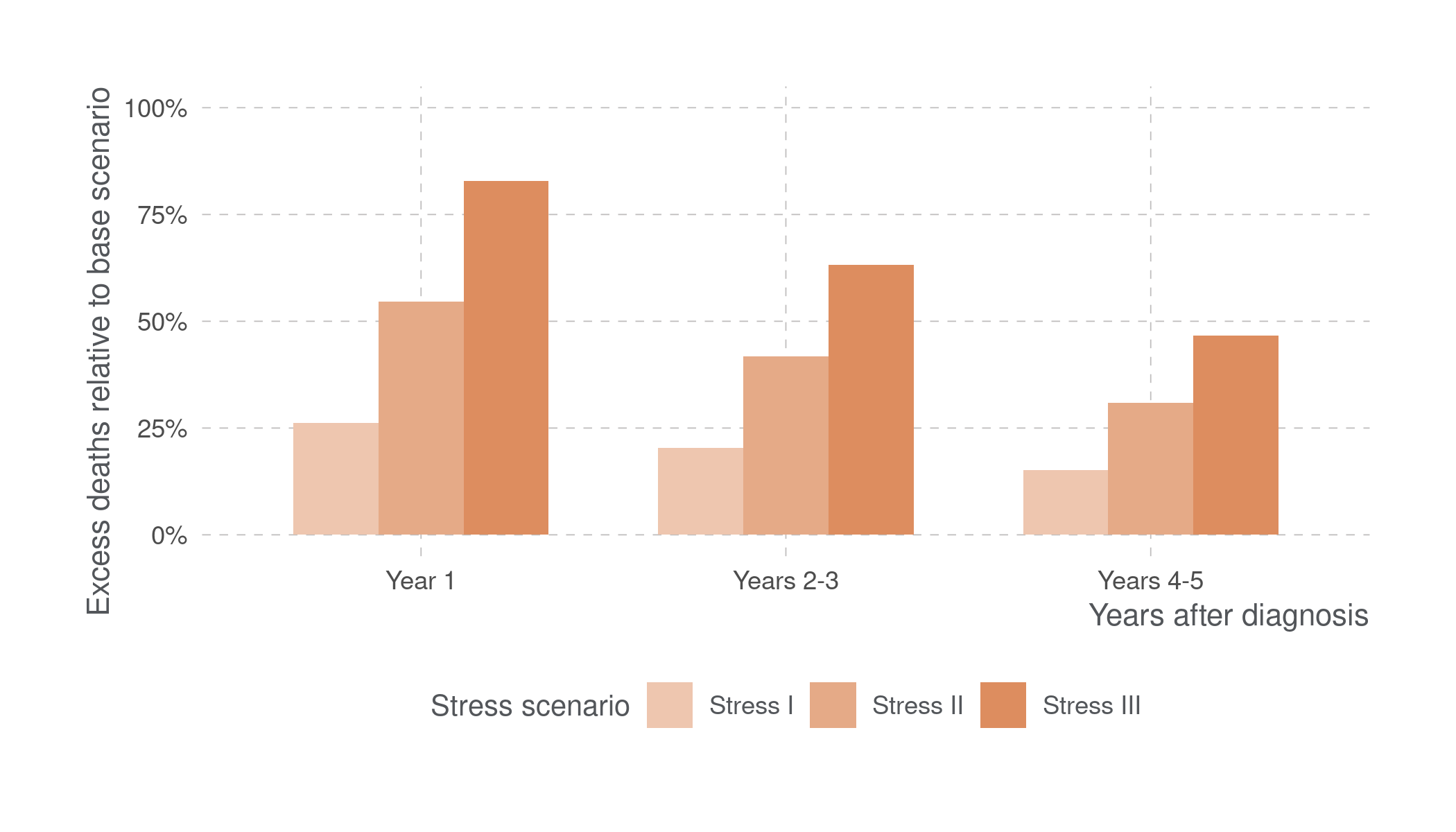 Figure 5: Mortality impact to a cohort of newly diagnosed patients after a single disruption year (2020). Mortality is above the base level even 4-5 years after diagnosis. Source: SEER7 and the American Cancer Society8 (data); PartnerRe (model analysis).
Figure 5: Mortality impact to a cohort of newly diagnosed patients after a single disruption year (2020). Mortality is above the base level even 4-5 years after diagnosis. Source: SEER7 and the American Cancer Society8 (data); PartnerRe (model analysis).